Article Text

Abstract
Objectives To explore the cost-effectiveness of a supervised moderate-to-high intensity aerobic exercise programme in people diagnosed with Alzheimer’s disease (AD) and estimate incremental cost-effectiveness ratios (ICER) using participant-reported and proxy-reported measures of health-related quality of life (HRQoL)
Design A cost-effectiveness analysis of economic and HRQoL data from a randomised trial delivered over 16 weeks.
Setting Memory clinics in Denmark.
Participants 200 individuals with mild AD aged 50–90 years gave informed consent to participate in the study. Participants were randomised to control or intervention group.
Interventions Control group received treatment as usual. The intervention group performed 1 hour of supervised moderate-to-high intensity aerobic exercise three times weekly for 16 weeks.
Primary and secondary outcomes measures Different physical, functional and health measures were obtained at inclusion (baseline) and 4 and 16 weeks after. HRQoL (EuroQol-5 Dimensions-5 Levels/EQ-Visual Analogue Scale) was reported by the participants and the primary caregivers as proxy respondents. Differences in HRQOL as reported by the participant and caregiver were explored as were different values of caregiver time with respite from care tasks.
Results The intervention cost was estimated at €608 and €496 per participant, with and without transport cost, respectively. Participants and caregivers in the intervention group reported a small, positive non-significant improvement in EQ-5D-5L and EQ-VAS after 16 weeks. The ICER was estimated at €72 000/quality-adjusted life year using participant-reported outcomes and €87000 using caregiver-reported outcomes.
Conclusions The findings suggest that the exercise intervention is unlikely to be cost-effective within the commonly applied threshold values. The cost of the intervention might be offset by potential savings from reduction in use of health and social care.
Trial registration number https://clinicaltrials.gov/ct2/show/NCT01681602.
- alzheimer’s disease
- cost-effectiveness
- quality of life measurement
- caregiver
- denmark
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This study uses data from a well-designed randomised controlled trial with near-complete data.
In this study, we investigate whether using EuroQol-5 Dimensions or EQ-Visual Analogue Scale has an impact of the cost-effectiveness of such an intervention using well-established methods.
The study had relatively short follow-up period and did not include cost consequences of health and social care used by the participants.
The study contributes to the discussion on whether health-related quality of life should be completed by patients or caregiver (as a proxy).
Background
Dementia is a group of common chronic brain diseases with over 80 000 cases in Denmark. This figure is projected to rise to over 140 000 over the next 30 years.1 Alzheimer’s disease (AD) is the most common cause of dementia and is characterised by memory problems, other cognitive impairments, and loss of daily functioning. The disease is progressive and has very serious physical and mental health implications for participants and caregivers, as well as significant socioeconomic impact, since most individuals with AD will need help and support from family members and from the public system.
Physical exercise may improve cognition, physical performance, functional ability and health-related quality of life (HRQoL) in people diagnosed with AD.2–5 Physical exercise, in particular, aerobic and resistance training in people with mild cognitive impairment has been shown to be cost-effective through reduction in healthcare use.6
Economic evaluation of physical exercise is challenging, as is evaluation of interventions aimed at individuals diagnosed with dementia. Some of these challenges relate to the measurements of outcomes or utilities. Measurement of utilities using the EuroQol-5 Dimension system (EQ-5D)7 is a frequently used standardised approach.8 However, one challenge facing such applications is that outcomes from interventions might not be measurable by the relatively crude instrument and outcomes may encompass other aspects than are included in the five dimensions of the instrument.
A further challenge arises with self-completion of health outcome measures. Completion of the EQ instrument is simple and many people find it an easy task. However, interpretation of health outcome measures completed by individuals with dementia may be more complicated as the disease may impair the respondents’ cognitive function and thereby impair the validity of the responses.9 It is possible to avoid this problem by asking the caregiver of participants with dementia to act as proxy respondents and complete the outcome measurements on behalf of or as supplement to the participant-completed measurement.10 However, use of proxy-completed outcome measures may not fully reflect the patients’ health-related quality of life (HRQoL) due to lack of first-hand experience.
In addition to the challenges of assessing the cost-effectiveness of physical interventions of individuals with dementia, some interventions may also produce positive externalities in the form of improved outcomes for the caregivers. That could be the case if an intervention gave the primary caregiver some respite from the caring responsibility. Such respite would arise if the individual with dementia was taken care of in another regimen on a regular basis (eg, a couple of hours a few times per week). In such cases, a discussion of whether such respite from care should be included and valued in an economic evaluation, and if so, to what extent, is pertinent.
The objective of this study was to explore issues relating to the assessment of cost-effectiveness of the intervention and estimate incremental cost-effectiveness ratios (ICER) using participant and proxy reported measures of HRQoL.
Method
Trial design
This study uses cost and HRQoL data from a previously published randomised trial.11 The primary outcomes of the 16-week follow-up period from baseline in cognitive performance (measured by Symbol Digit Modalities Test (SDMT)) and secondary outcomes as changes in other cognitive measures, quality of life, abilities to perform daily activities of daily living and neuropsychiatric and depressive symptoms have been reported,12 as well as the effect on physical performance.13
Briefly, the trial entitled ‘Preserving Cognition, Quality of Life, Physical Health and Functional Ability in Alzheimer’s disease: the Effect of Physical Exercise (ADEX)’ was a multi-centre randomised trial conducted In Denmark between January 2012 and June 2014. Participants with mild AD (Mini-Mental State Examination (MMSE) score≥20) aged between 50 and 90 years were randomised to a control group that received treatment as usual, or an intervention group which performed 1 hour of supervised moderate-to-high intensity aerobic exercise three times weekly for 16 weeks.
The intervention exercises were conducted in groups of 2–5 participants, supervised by an experienced physiotherapist. The first 4 weeks aimed at building strength of the lower extremities and introduced aerobic exercise. The remaining 12 weeks, participants performed aerobic training on bicycle, cross trainer and treadmill. The target intensity was 70%–80% of maximal heart rate. The control group received treatment as usual, and was offered a 4-week adaptation exercise programme after the termination of the study.
The study was approved by the Danish National Committee on Biomedical Research Ethics (reference number H-3-2011-128) and by the Danish Data Protection Agency (J No. 30–0718).
Overview of the cost-utility study
We used the Danish healthcare perspective and included the time use of participants as complementary outcome description. The analysis was restricted to a 16-week time horizon.
Health outcomes
Relevant measures of outcomes for this cost-utility analysis included the Danish version of EQ-5D-5L and EQ-Visual Analogue Scale (VAS).7 The instrument was administered to both the participants and their caregivers as proxy respondents. The available EQ measurements included data from baseline and 16 weeks completed by participants and caregivers in control and intervention groups. The descriptive categories of the EQ-5D-5L were converted to utilities using the available international scoring algorithm.14 We calculated quality-adjusted life years (QALYs) for each individual participant using the participant and proxy-respondent scores.
Cost outcomes
Costs related to the intervention were recorded monthly for each individual, and were based on participants’ compliance with the training programme as recorded by the physiotherapist responsible for the group training. The questionnaires administered to participants and caregivers recorded the time spent at the training sessions by the participants and their caregivers, as well as the mode and cost of transport to and from the sessions.
The estimation of average cost per participant was conducted by a top-down and bottom-up approach. The top-down approach costed staff resources allocated to each memory clinic during for the whole project using standard salaries. The cost of participants’ transportation was obtained as records made in the memory clinics’ accounting systems. In addition, the participants’ fees paid to the clinic from the project were assumed to cover the cost of the training facilities and ancillary staff. The bottom-up cost assumed a cost per training session attended estimated based on an hourly group training session with four participants and average cost for clinic organised transport of participants.
We calculated the total programme cost for the full programme and estimated the average cost per participant (top-down) and the individual cost using the average cost per attended training session (bottom-up).
Participants’ and accompanying persons’ time use was estimated as the duration of the training (60 min) with addition of 30 min for preparation and changing before and after the training and 30 min transport.
The cost analysis excluded the value of participants’ and caregivers’ time, their private transport costs and other private costs. The cost analysis also excluded potential costs relating to accidents/adverse events during the training sessions and changed demand for healthcare—for example, in primary and social care.
Costs were collected and recorded in 2015 Danish Crowns (DKK) and are reported in 2015 Euro (€) (€1=7.46 DKK). Discounting was not applied due to the short 16-week time frame.
Missing data
Missing data were not a serious problem. For five participants, the number of attended training sessions was missing and replaced with the relevant 4-week period mean of the available data. Mode of transport was missing for 31 out of 3966 training sessions (0.7%) and was assumed to use other transport. Ten participants did not provide valid EQ-VAS or EQ-5D-5L at follow-up. No replacement was made for these data. Logistic regression did not identify any characteristics with statistical significant differences between those with and without follow-up EQ-data.
Analyses
The average number of hours spent on exercise was estimated based on the data reported by the physiotherapist. Participants completing the entire exercise programme with high intensity were analysed separately as a per-protocol group.
Use of caregivers’ time was obtained from the self-completed questionnaires where it was indicated whether the participant attended the exercise group accompanied by the caregiver. Mode of transport was also obtained from the questionnaires and was used to estimate the total time of transport. Although different cost estimates were available, the analyses reported here used only the direct cost of the training programme excluding transport costs. This was the lowest cost estimate and the other estimates would provide higher cost-effectiveness ratios than reported here. The choice of the lowest cost estimate may be justified as a realistic assessment of the resource use when the intervention is provided on a routine basis and in particular if the training is provided by private organisations with agreement by the municipal purchasing authorities.
The available EQ-data were analysed using both the participants’ and caregivers’ assessment. Differences at baseline were assessed by graphical box plots and estimated association between assessments. The Pearson correlation coefficient between the participant and caregiver assessment was estimated separately for the control and exercise group. Variables were assessed for normality using visual examination and the Shapiro-Wilk test. In addition, the difference in health status between the baseline and follow-up assessment by the participants were assessed graphically and by Pearson correlation coefficients. Analysis of the raw EQ-data was conducted using parametric mean values and the associated 95% CIs. Baseline differences between groups were estimated using ordinary least squares (OLS) regression with dummy variables for the exercise group or caregiver as only independent variables.
Difference-in-difference estimates were also based from OLS regression. Three types of estimations were made: measures of incremental changes (=follow-up—baseline) with exercise group as the only independent variable, with baseline scores as an additional variable and with a number of social variables (gender, age, civil status, MMSE score, Hamilton’s Depression score and two physical scores).
Incremental cost-effectiveness ratios were calculated using the baseline-adjusted estimates for EQ-5D-5L. Bias corrected and accelerated bootstrap methods were used to derive 1000 sets of estimates for incremental cost and EQ measures. These estimates where used to construct cost-effectiveness acceptability curves (CEAC) showing the probability of the exercise intervention being more cost-effective than the controls for different maximum levels that the decision makers may be willing to pay for an additional QALY.
CEACs were estimated using the subsample of participants who had been compliant with the intervention in comparison with the control group.
To assess the potential consequences of assigning different values of respite time values within the range of €0–€10 per hour was used. In this assessment, the net cost of the exercise was estimated by deducting the value of the time that the participant attended the exercise programme (including preparation and transport).
Stata V.14.1 was used for all analyses. p Values <0.05 were considered statistically significant.
Results
Participants
A total 608 potential participants were assessed for eligibility in the duration of the programme. Of those, 104 did not meet the inclusion criteria, 107 declined to participate and a further 197 had transport problems or were excluded for other reasons. A total 200 individuals were randomised to the intervention group (n=107) or the control group (n=93) (see online supplementary table 1). After 16 weeks, 102 from the intervention group and 88 from the control group provided data for the duration of the study, resulting in a loss to follow-up of five from each groups.12 There were no statistical significant differences in baseline characteristics between the two randomised groups.12 The drop-out rate was 4% and 8% for the intervention and control groups, respectively.12
Of the 200 randomised participants, 57% were male. Mean age was 70.02 (SD 7.41) years and the mean MMSE score was 23.96 (SD 3.59). Of the 107 participants in the intervention group, 76% attended more than 80% of the exercise sessions and 78% (n=66; analysed as a per-protocol group) exercised with an intensity of more than 70% of the maximal heart rate.12 No significant differences in background characteristics could be found between participants in the control group and the low-intensity and high-intensity exercise group.12
Resource use and cost outcomes
Participant time
During the 16-week period, the group of 107 participants in the exercise group had in total 3966 training sessions and used in total 7932 hours on participating in the programme. That corresponds to an average of 37 training sessions (median 41; max 47) and 74 hours of training, change and transport (median 82 hours, max 94 hours). Forty-nine of the participants arrived to the training with an accompanying person, and they used in total 2120 hours corresponding to 43 hours per accompanied participant or 20 hours per participant. The average time used for participants at different memory clinics is presented in online supplementary figure 1.
Top-down cost
Each Memory Clinic were allocated financial coverage of 0.5 full-time equivalent (FTE) physiotherapist, and 0.6/0.75 FTE nurse from research programme. The clinics funded the transport cost for the participants who required transport assistance (~€80 000) out of their own budget. In addition, the clinics were paid from the research programme €135 per active participant per 4-week training. The total programme cost was estimated at €429 000 resulting in an average programme cost per participant at €3990.
Bottom-up cost
Assuming that one physiotherapist provided 1 hour training group sessions with four participants, the average cost per participant per session was estimated at €13. Hospital-provided transport cost was estimated at €82 per participant per session (970 sessions).
The average incremental cost for participants in the exercise group was estimated at 608 (95% CI 604 to 612) and 496 (95% CI 495 to 497) with and without transport cost, respectively.
EQ measurements
Baseline and follow-up (16-week) measurements were reported by participants and their caregivers and were measured using EQ-5D-5L and EQ-VAS. At baseline, all participants (control and intervention) reported a mean score of 0.929 (95% CI 0.916 to 0.942) and 83.2 (95% CI 81.2 to 85.3), as measured by EQ-5D-5L and EQ-VAS, respectively. Caregivers reported a mean score of 0.864 (95% CI 0.847 to 0.882) and 73.7 (95% CI 71.2 to 76.2). No statistically significant baseline difference was found between the control and exercise groups for any of the measurements.
The intervention yielded a statistically significant increase over time in EQ-VAS assessed by the caregiver (3.8; 95% CI 0.2 to 7.4), indicating a 3.8 point improvement (on a 100-point scale) in caregiver-completed HRQoL measure. All other measures indicated insignificant positive changes 16 weeks after the baseline measurement with the change scores for the exercise group being consistently larger than for the control group. An overview of baseline and follow-up EQ-5D-5L and EQ-VAS measurements by participants and caregivers is presented in online supplementary figure 2.
The correlation between participant-reported and caregiver-reported quality of life as measured by EQ-5D-5L and EQ-VAS is presented in figure 1. The black lines indicate identical health status assessment, while points below the black line indicate that the caregiver is assessing the participants’ health status worse than the participants themselves. The blue and red lines correspond to the estimated relationship (linear regression) between participants’ and caregivers’ assessment in the control and exercise group. Using the EQ-5D-5L, 54% of the caregivers reported a worse health state than the participants at both baseline and after 16 weeks, while 26%–29% indicated similar and 17% and 19% indicated better health states. Using the EQ-VAS the caregiver’s assessments were worse than the participant’s in 62% and 68% of the cases and better in 26% and 23% of the cases. The estimated correlation coefficients were 0.29 (p<0.001) and 0.24 (p<0.001) for baseline and 16-week assessments, respectively, for EQ-5D-5L, Correlations were weaker for EQ-VAS, resulting in correlation coefficients of 0.16 (p<0.001) and 0.19 (p<0.001) at baseline and 16 weeks, respectively.
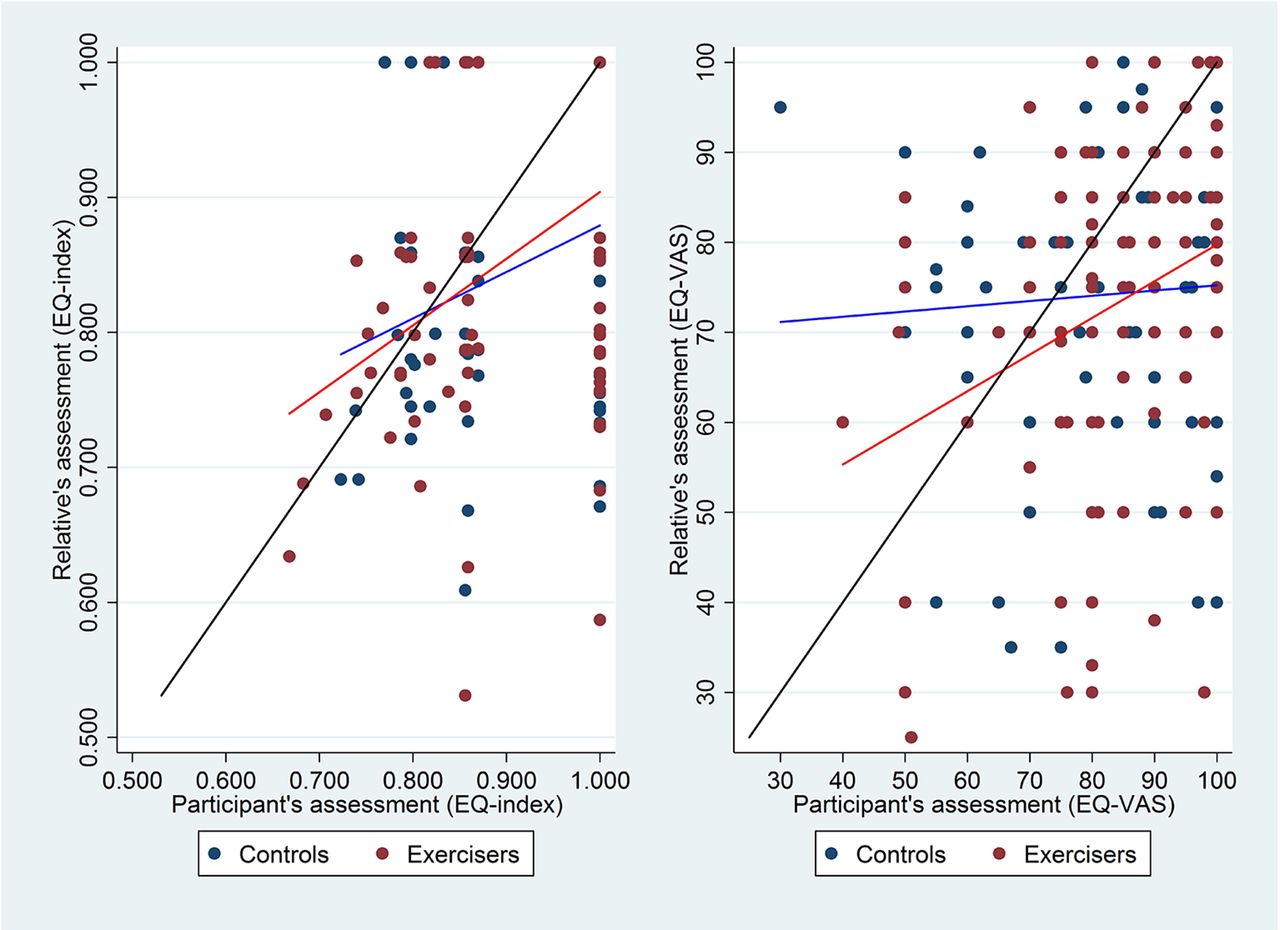
Correlation between participants’ and caregivers’ assessment of baseline EQ-VAS and EQ-5D-5L converted to index values. EQ-5D-5L, EuroQol-5 Dimensions-5 Levels; EQ-VAS, EQ Visual Analogue Scale.
The change over time in participants’ measurements is illustrated in figure 2. The black line indicates identical health status assessment at baseline and 16 weeks after. Points above the black line indicate that the participants reported better 16 weeks health status than at baseline. The blue and red lines correspond to the estimated relationship (linear regression) between participants’ assessment at baseline and at 16-week follow-up. It appears that the correlation between the participant-reported measurements are stronger correlated with the EQ-5D-5L (0.59, p<0.001) than the EQ-VAS (0.51, p<0.001), and that the correlation is stronger for the exercise group than the control group (0.72 (p<0.001) vs 0.41 (p<0.001) (EQ-5D-5L)).

Correlation between participants’ baseline and 16-week follow-up assessment of EQ-VAS and EQ-5D-5L health status converted to index values. EQ-5D-5L, EuroQol-5 Dimensions-5 Levels; EQ-VAS, EQ Visual Analogue Scale.
EQ difference-in-differences
Four baseline-adjusted estimates for difference-in-differences were estimated using the EQ-5D-5L utility index and the EQ-VAS as provided by the participants and proxy respondents. The participant assessed EQ-5D-5L difference was estimated at 0.002 (95% CI 0.005 to 0.009; p=0.59) and the proxy assessed difference at 0.005 (95% CI 0.004 to 0.014; p=0.24) which does not indicate support for utility gains from the intervention. Using the EQ-VAS score, the participants’ assessment indicated a difference of 0.62 (95% CI 0.61 to 1.85; p=0.33) and 0.45 (95% CI 0.88 to 1.77; p=0.51) when using the caregivers’ assessment. Estimations adjusting for baseline score, demographic, social and health characteristics provided slightly larger, but still insignificant differences.
Incremental cost-utility ratio
Using the participant assessed EQ utility index and cost excluding transport costs the ICER was estimated at €158 520/QALY and 120 790 using the proxy-reported EQ-5D-5L index.
Using the EQ-VAS the ICER was estimated at €72 120/QALY using participants’ EQ-VAS-5D and €87 157/QALY using the caregivers’ EQ-VAS. The scatter plot of the participant-reported EQ-5D-5L is illustrated in figure 3.

Scatter plot ICER using participant reported EQ-index. EQ, EuroQoL; ICER, incremental cost-effectiveness ratios.
The cost-effectiveness acceptability curve using the four different measures of health is illustrated in figure 4. There is a 50% chance of the intervention being cost-effective using participant EQ-5D-5L at the threshold value of €175 000/QALY. With the participant-reported EQ-VAS, the threshold value is reduced to €75 000 . When using caregivers’ scores on both EQ-5D-5L and EQ-VAS, threshold values lie between €120 000 and €70 000, respectively.

Cost-effectiveness acceptability curve using different measures of health status index. Based on data from intention-to-treat analysis. EQ-5D-5L, EuroQol-5 Dimensions-5 Levels; EQ-VAS, EQ Visual Analogue Scale.
As previously described, adherence to exercise protocol was achieved by 66 participants. When we restricted the analysis to these individuals (ie, per-protocol analysis), the cost-effectiveness acceptability curves shift (figure 5). Both participant-reported threshold values are lower than caregiver-reported results. Further, both caregiver and participant EQ-5D-5L measures resulted in higher thresholds than VAS measures. With increased adherence to protocol, both EQ-5D-5L and EQ-VAS measures by participants yielded a lower threshold than for all participants.

Cost-effectiveness acceptability curve comparing participants with high-intensity exercise (n=66) with controls. Based on data from per-protocol analysis. EQ-5D-5L, EuroQol-5 Dimensions-5 Levels; EQ-VAS, EQ Visual Analogue Scale.
The exercise programme provided caregivers with respite from caregiver tasks. We considered a range of values of this free time—from €0 to €10/hour. Figure 6 demonstrates the probability of the intervention being cost-effective (with quality of life measured by the participant-reported EQ-5D-5L) across this range. The intervention is considered cost saving when we value the caregiver time above €10/hour.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Sensitivity analysis with different values of caregivers’ respite time.
Discussion
In the general population, physical activity may have a positive impact on health and health-related quality of life. Physical activity may also provide important health impacts to people diagnosed with dementia.15 Having established positive relations to health, it becomes relevant to consider whether certain interventions can ensure that more people with dementia become physically active. Therefore, it is relevant to assess whether such interventions actually improve the health of these people (and their caregivers). It is also relevant to investigate whether such interventions are ‘worth it?’.16 17 A number of economic evaluations have already been conducted and summarised in systematic reviews.18 However, economic evaluation of interventions aimed at changing behaviour in the elderly population is challenging.19 In particular, challenges lie in ensuring reasonable compliance with the intervention programme, defining valid outcome measures and acquiring realistic assessments of such outcome measures. In addition, a discussion of who may benefit from the intervention arises. Clearly, if high compliance can be achieved, the participants may benefit from both the process and outcomes, but benefits of an intervention may also extend to participants’ caregivers. That may indeed be the case with people with AD, where the informal caregiver may perceive temporary relief from the tasks of caring for the participant.
This cost-utility study was based on a carefully designed and conducted clinical trial of providing an intensive physical training intervention programme to people with mild AD. For the application in the cost-utility analysis, standard measures of resource use and health outcomes were collected from each participant. These data were analysed according to current analytical standards. However, it became clear that some methodological choices have impacts on the results. Thus, the standard assessment of the cost-effectiveness of the intervention provided an ICER of €160 000/QALY, which is clearly not very attractive but also not without the reach of providing ‘good value for money’ in a Danish context.
Challenges for the ICER result
It is clear that the ICER depends on the incremental cost and outcomes, and, indeed, the time frame that these are considered.
Cost
The cost analysis included the programme cost but disregarded potential consequences in the demand for health and social services. The time perspective of such data collection for further cost analysis would ideally be longer term (eg, 12 months after the intervention began). However, given the age group and nature of the disease there could have been expected a considerable deterioration in the health states of participants and a relatively high risk of mortality. As healthcare cost increase with proximity to death, there would be strong concerns of the validity of the association of potential cost differences and the intervention. The cost analysis in this study is dependent on the nature of this exercise intervention, and a different intensity or frequency of exercise may have yielded a different cost result.
Several other cost items could have been included. Complications or accidents due to the physical exercise intervention would be one that potentially would increase the cost of the exercise group. A few accidents and other complications appeared during the study period.(7) Some minor adverse events were likely related to the intervention, that is, musculoskeletal problems, but only one serious adverse event (atrial fibrillation) was possible linked to the intervention. The statistical power of the study was probably too weak to accurately identify such complications and their cost consequences due to the intervention.
Another cost aspect that was considered was a reduction in the demand of social services and delays in movement to nursing home. The hypothesis was that participants in the exercise group could remain more self-sufficient at their homes for longer time. If such hypothesis was true, that would mean that the intervention would be able to provide potential cost saving to the municipal social service and nursing home provision. However, the collection of municipal service data would require a considerable effort as such data are not collected in a standardised way or recorded in national databases. The movement into nursing homes was considered collected by phone contacts to the caregivers. However, such indicators would not only indicate effect of the intervention but are also influences of the local capacity and demand for nursing home, and are thus heavily influenced by organisational factors in the different municipalities. Interpretation of differences in (time to) move to nursing homes was therefore perceived to be a weak indicator although in principle relevant.
In the cost-utility calculation, a simple measure of the intervention cost was used dependent on the number of training sessions each participant attended and an associated unit cost. The top-down costing analysis provided a much higher average cost estimate, but part of the funded resources were used to plan and conduct the evaluation and would therefore not be relevant for the cost-utility estimates.
Outcome measurements by the EQ instrument
The EQ instrument has been assessed for applications with people diagnosed with dementia.20–23 A recent study concluded that the EQ-5D-5L might have advantages over dementia-specific measures such as DEMQoL and QoL-AD, and that it can be used as a stand-alone measure of quality of life in dementia research.20 The effects of the current intervention may be of a nature that is difficult to capture. Certainly, the clinical reports on this trial indicated that the usual dementia outcomes measures were unable to identify strong clinical changes.12 However, cardiorespiratory fitness and exercise self-efficacy improved significantly, and per-protocol analyses showed improvements in both single-task physical performance and dual-task performance.13 Some evidence suggests that the EQ-5D-5L instrument is more responsive to physical aspects of health in elderly, whereas DEMQOL is more responsive to cognitive changes.24 Perhaps concurrent use of multiple HRQoL instruments may aid in capturing the full effect of exercise interventions.
The outcomes measured by the EQ instrument indicated an incremental change of 0.007 using the EQ-5D-5L and 2.0 using the EQ-VAS. These mean measures hide the fact that some participants actually reported better health status at 16-week follow-up than at baseline, suggesting a health improvement and that some reported health deterioration or no change. It is unclear whether the observed changes would be within the range of minimal meaningful clinical difference.25–28
In the analysis, participants who fully complied with the exercise intervention the outcomes appeared to be better in comparison with the whole control group (figure 5). However, the intervention may have a positive lasting effect on the objectives of preserving cognition, improving quality of life, physical health and functional abilities—which may not be captured by the EQ-5D-5L instrument. If this is the case, then the effects of the intervention are underestimated. It is also important to recognise that participants of this study were willing and able to participate in intensive exercise, which may not be representative of the general AD population. It is possible, that this programme may be more beneficial for people with lower levels of cognitive impairment or more sedentary lifestyles.
Proxy measurements
Due to the cognitive impairment of dementia, it may be difficult to obtain self-completed measurement and, indeed, to trust the validity of the self-completed measurements. Therefore, it is common practice to obtain proxy measurements from caregivers on behalf of participants. This raises the issues as to what extent caregivers are able to validly assess the health status of the participants, and how to handle possible discrepancies between the responses by the participants and proxy respondents.29 30
It appears that the probability that the intervention is cost-effective in comparison with the control is higher when using participant assessments than the caregiver assessment (figure 4). It is interesting to note in the per-protocol analysis of participants, who fully complied with the exercise intervention that the CEACs using the caregiver-reported health status appeared to indicate substantial lower probability for cost-effectiveness than the participant-reported health status (figure 5). This may need further exploration.
Valuation of respite from care
In the analysis where the value of caregivers’ respite was used to offset the cost of the intervention, a fairly low time value (below €10/hour) indicated that there was a high probability that the intervention would be cheaper and more effective (figure 6). However, when a positive value was assigned to an EQ gain, the probability of the intervention being cost-effective reduced. This relates to the fact that not all participants in the exercise group achieved a gain in EQ score and, thus, the saving from the intervention cost and value of respite from the caring task should be off-set by the apparent loss in EQ score.
Conclusion and perspectives
The trial design with randomisation to control and intervention group and the availability of nearly complete data are the main strengths of the study. The cost-effectiveness analysis was conducted using standard analytical methodologies and has tested the consequences of different methodological challenges.
The relatively short time perspective and perhaps lack of data about the cost consequences of health and social care are potential weaknesses. If the effect of the intervention is expected to last for a period beyond the 16 weeks follow-up, then the outcomes might be underestimated, and thus the probability of the intervention being cost-effective might be underestimated.
In future studies, the longer term effects in terms of additional resource use and longer term health improvement might be considered.
This analysis suggests that the exercise intervention may not be cost-effective under commonly used threshold values for health gains. This would indicate that municipalities, who are responsible for providing rehabilitation services to people with dementia, should consider ways of providing the intervention at a lower cost or, perhaps, to a more targeted group. One concern that might especially be addressed is how such a programme may achieve such high completion rates as was obtained in this study. When implemented in daily practice, such rates may be expected to reduce as the target group will be expanded and thus include individuals who are less motivated for physical exercise or are less supported for such activities by their caregiver.
Acknowledgments
We are thankful to all the physical therapists, nurses, clinical raters and investigators for their contributions to the ADEX study. Memory clinic investigators: Birgitte Bo Andersen, MD, DMSc, , Dept. of Neurology, Rigshospitalet (Blegdamsvej), University of Copenhagen; Peter Høgh, PhD, MD, Roskilde Hospital Memory Clinic; Vestergaard, MD, Aalborg Hospital Karsten; Hans Brændgaard, MD Hanne Gottrup, PhD, MD, Aarhus University Hospital; Anette Lolk, Associate Professor, PhD, MD Lene Wermuth, MD, Dementia Clinic, Odense University Hospital; Søren Jakobsen, MD, Department of Geriatrics, OUH, Svendborg Hospital; Lars P Laugesen, MD Robert Graff Gergelyffy, MD, Department of Geriatrics, Slagelse Hospital; Eva Bjerregaard, MD,Dept. of Neurology, Rigshospitalet (Glostrup) University of Copenhagen
References
Footnotes
Contributors GW, SGH, NB contributed to the design of the trial. SGH was the principal investigator of the trial. NB was responsible for the physical assessments and the physical exercise intervention. JS conducted the economic analysis with help from ES. GW contributed to interpretation of the data. ES and JS drafted the paper. All authors participated in writing the paper, reviewed it for content and approved the final version.
Competing interests None declared.
Patient consent Not obtained.
Ethics approval Danish National Committee on Biomedical Research Ethics.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data is not available for sharing
Correction notice This paper has been amended since it was published Online First. Owing to a scripting error, some of the publisher names in the references were replaced with 'BMJ Publishing Group'. This only affected the full text version, not the PDF. We have since corrected theseerrors and the correct publishers have been inserted into the references.